

Locals had seen nightmares like this before washed up on the beach. The Natives called these monsters “omajinaakoos” or “The Ugly Ones”, believing they were omens of bad luck. The locals knew these strange creatures were just the result of animal experiments gone wrong. Experiments being conducted on nearby Plum Island.
Not far from that eerie discovery lies a piece of land just off the north fork of Long Island. A government owned property for research called Plum Island. The locals whispered in conspiracy circles about the Plum Island Animal Research Facility as a hotbed of secretive government experiments. During the Cold War, it was said to be the center of research into weaponized pathogens and disease-carrying insects. And just across the Long Island Sound sits Lyme, Connecticut—ground zero for a mysterious outbreak of a disease that would come to bear its name.

Coincidence? We don’t believe in those anymore, do we?


What? Too soon?
The pathogen responsible for Lyme is no ordinary microbe. Many claim it is the product of an experiment gone awry. Who was running these experiments on tick borne pathogens? Ones that sound strangely like the gain of function we’ve become all too familiar with in recent years? Enter a gentleman by the name of Dr. Erich Traub. A German virologist recruited to the U.S. to help with animal infection research. What was Traub’s specialty? Infecting ticks with dangerous pathogens. And where did he end up? Plum Island.
I didn’t used to believe in conspiracy theories, but… Where’s our body count at now? How many times? Covid, UFOs, MKUltra, free energy? The truth can only be covered up and lied about for so long. People aren’t stupid. We can do our own research.
https://www.youtube.com/watch?v=AwRQh1NZ4Sc
I love that bit. Thank you Jimmy Dore.
The Horrors of Plum Island
Founded in 1910, Reims Island in Germany is home to the oldest virus research facility in the world. During World War 2, Riems became ground zero for Hitler’s biowarfare program – run by German veterinarian, scientist, and virologist Dr. Erich Traub. Traub worked directly under SS Heinrich Himmler, Adolf Hitler’s second in command – after receiving his fellowship from the Rockefeller Institute for Medical Research in Princeton, New Jersey, where he perfected his skills in viruses and vaccines before returning to Germany.
There, he took a particular interest in developing a specific kind of biowarfare. Biting insects – specifically infecting biting ticks with diseases aimed at crippling not just one enemy soldier but an entire population. After the war, Traub was, like many Nazi scientists, trapped in the iron curtain of Soviet-occupied Germany.
Along with 1600 other German scientists, Traub was identified as a ‘high priority intelligence target” by US intelligence. He was evacuated by the British government and brought to the United States under the auspices of a secret program called Operation Paperclip. Operation Paperclip was a government program designed to exploit scientific knowledge of Nazi German scientists. Instead of information on biowarfare falling into the hands of the Soviets, it would become possession of the United States. In other words, instead of being tried for his war crimes, Nazi scientist Dr. Erich Traub came to work for us.
Erich Traub (27 June 1906 – 18 May 1985), German veterinarian, scientist and virologist
Traub specialized in biting insects and was initially sent to Fort Deitrich to study…well, we’re just not sure. Little is known about his clandestine research, although the names of a few studies have been pried out under FOIA requests. We know that Traub studied over forty different lethal viruses on animals at Fort Dietrich. He continued his research on ticks, a vector considered ideal for biological warfare. Diseases spread by ticks could destroy entire populations of people and animals without firing a single shot.
After his work at Fort Deitrich, Traub was promoted to a new lab – One located just off the Long Island peninsula of NY. The now infamous Plum Island Animal Disease Center. By the mid-1950s, he was stationed at Plum Island, where rumors suggest he was involved in researching how ticks could be used as vectors to spread pathogens. Pathogens like one discovered – or developed – by Swiss scientist and US bioweapons expert, Dr. Wilheim Burgdorfer. More on that in a bit.

Fast-forward to the 1970s. Just miles from Plum Island, in the small town of Lyme, Connecticut, children and adults began developing strange symptoms—rashes resembling bullseyes, severe joint pain, fatigue, and neurological issues. In 1975, two mothers from Lyme, Polly Murray and Judith Mensch, pushed for answers when dozens of cases clustered in their small community.
This was the first documented outbreak of what we now call Lyme disease. Some argue that Traub and Burgdorfer’s mid-century experiments with tick-borne diseases set the stage for this outbreak that would surface decades later. The proximity, the timeline, the Nazi scientists —it all feels just a little too convenient.
How Lyme First Presented
It started quietly. Polly Murray, a painter and mother of four, began experiencing debilitating symptoms—fever, muscle aches, and swollen joints that seemed to come out of nowhere. Soon, her children fell ill with similar complaints, and she began to notice that her neighbors were reporting the same thing. Rashes shaped like bullseyes appeared on the skin of some. Others, without the rash, suffered mysterious neurological symptoms that left doctors perplexed.
Frustrated by the lack of answers, Polly reached out to Yale researchers, who eventually connected the illness to deer ticks and identified the bacterium Borrelia burgdorferi as the culprit. But even then, there were questions. Why here? Why now? And why did this bacterium seem so adept at outsmarting the immune system?
Lyme disease isn’t just another bacterial infection. It’s caused by Borrelia burgdorferi, a pathogen that defies categorization. And one boldly named after the Swiss scientist Wilheim or ‘Willy’ Burgdorfer, who “discovered” the pathogen in deer ticks.
Shortly before his death in 2014, he admitted that Borrelia was indeed the rest of biowarfe research gone wrong. Basically. Kind of. He had advanced Parkinson’s disease at the time, so it’s a little difficult to make out his exact words. There are several books and documentaries on this. You be the judge.
Unlike most bacteria, Borrelia can shapeshift from a twisty spirochete into a stealthy biofilm. The alterations in surface proteins from one form to the next allow it to easily evade and, in time, suppress the immune system. Its spiral shape allows it to burrow deep into tissues, and its behavior mirrors that of a terrifying virus.
There are a few infections that medicine has largely failed at managing. Why? Well, perhaps it’s because they don’t behave like anything that’s evolved naturally. From nature. Think about the times in your life you gotten a stomach flu? You crap your pants and puke your brains out for a day or two and it’s over. Influenza? Fever, body aches, cough, a few days off from work and you’re back at it. We know what to expect from these bugs.
But what’s with these infections with strange symptoms that seem to affect every organ system and then linger on into oblivion? Take Covid for example. No smell, no taste, heart palpitations, brain fog, depression, joint pain. And that’s on the front end. Infection comes and goes and somehow these bugs are still causing debilitating long term symptoms? Well, that’s not normal. We’ve obviously seen this with Covid – that was 5 years ago and countless people are still suffering with ‘Long Covid’ symptoms.
I’m going to argue that Covid wasn’t the first lab escapee unleashed on the world’s population. Since the 1970’s countless humans have been devastated by another completely unnatural beast – Lyme. Our health authorities say Lyme disease can easily be treated with 10-14 days of antibiotics. That’s what we’re taught in medical school anyway. So, who are all these patients with ‘Chronic Lyme’? Many took the obligatory antibiotics but never got better. An outsider might be hard pressed to tell the difference between Long Covid and Chronic Lyme. Two distinct organisms – both benefiting from some function that has been gained? You tell me.
The conventional system says Chronic Lyme does not exist. Fibromyalgia exists. As does chronic fatigue syndrome, Multiple Sclerosis, and POTS. But not Chronic Lyme. Untold numbers of Americans are debilitated by these ‘diseases. But what if they’re all caused by the same underlying problem? The persistence of a completely unnatural pathogen? Let’s get into it.
https://www.cdc.gov/lyme/treatment/index.html
What is Chronic Lyme?
Chronic Lyme is a complete garbage bag of symptoms caused by the persistence of an organism that may or may not have been engineered in a lab. Fatigue, brain fog, numbness and tingling, skin rashes, psychological disturbances, gut dysfunction, muscle weakness, sleep disorders, dysautonomia or ‘I get lightheaded or pass out when I stand up’. We believe this happens for a number of reasons, including but not limited to the following:
- Acute infection was missed and not treated with antibiotics.
- Acute infection was caught, treated, but genetics or other factors did not allow for immune system to clear the infection.
- Acute infection was never suspected because symptoms were…zero.
- Infection was never susceptible to antibiotics to begin with.
Seemingly by design, or lab engineering, the ticks that carry Lyme rarely just carry Lyme. They’re packed with other beasts. More often than not, they also carry other horrifying infections – Bartonella, Babesia, Anaplasmosis, Ehrlichiosis, Rocky Mountain Spotted Fever, Mycoplasma – a whole host of fun.
Until it isn’t. Even the conventional system recognizes that in some cases, Lyme disease doesn’t behave as expected. Even with antibiotics. Some people get a specific kind of rash, others go on to have Bell’s palsy or even encephalitis. Others never remember even having had an initial infection to begin with, but their blood work says otherwise. Why do some people seem to recover uneventfully from Lyme, and others go on to suffer a lifetime of misery?
Cue the conspiracy theorists.
Regardless of whether you believe Lyme was the result of genetic engineering or a lab leak, the fact remains that it is a beast of a pathogen. It can affect any organ system. It is almost impossible to detect on a regular blood test unless caught extremely early in the course of illness. It suppresses the immune system, making it extremely difficult for its host to not just defend itself against the Lyme – but other infections as well. This immune system dysregulation opens the door to other major problems like autoimmune disease and cancer. It affects men, women, and children of all ages and presents differently in everyone.
How Do I Know If I Have Lyme?
This is tricky because conventional testing has extremely poor sensitivity for finding it – and this is the only testing your doctor will ever do. Because it’s the only testing they believe exists. The conventional testing measures a person’s response to the Lyme infection by measuring something called antibodies. When your immune system sees a virus or bacteria, it makes something called antibodies to fight it off. Well, it’s supposed to, anyway.
But if the infection we’re measuring is extremely adept at suppressing the immune system, can we trust a negative test? We’re 50 years away from the mid-1970s and, thankfully, have many more sensitive testing options for Lyme available. Ones that can test for the organism itself as well as amplify the signal that says your body saw something that looks like Lyme. Of course these aren’t yet covered by insurance, and regular docs typically aren’t familiar with them at all.
As far as symptoms are concerned, these are all over the map. Often people with Chronic Lyme have seen a lot of doctors. A LOT of doctors. They’ve spent a lot of money. Like a crap ton of money. Taken a lot of medications. Done a lot of their own research but haven’t got a lot of answers.
- Fatigue
- Cognitive difficulties
- Neurologic symptoms
- Mood changes
- Sleep disturbance
- Joint and Muscle Pain
- Heart issues
- Difficulty regulating blood pressure and heart rate (POTS/dysautonomia)
- Autoimmune diseases
- Multiple Sclerosis
- Rheumatoid arthritis
- Psoriatic arthritis
- Systemic lupus erythematosus (SLE)
- Sjögren’s syndrome
- Dermatomyositis
- Hashimoto’s thyroiditis
- Polymyalgia rheumatica
- Autoimmune neuropathy
- Guillain-Barre syndrome
- PANS (Pediatric Acute-onset Neuropsychiatric Syndrome)
- PANDAS (Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infections)
Even with a diagnosis – which is hard to get – fixing the problem has historically been even harder. If you’re fortunate enough to fall into the category of catching Lyme super early and treating it with antibiotics that work, you might be in the clear. For my patients with Lyme, they’re typically not so lucky.
Historically, we’ve tried the ‘kitchen sink’ approach when ‘Chronic Lyme’ is identified or suspected.
- More antibiotics
- Different antibiotics
- Combinations of antibiotics
- Immune system support
- Stem cells
- Binders and Detoxification
- Crossing our fingers
- Rubbing a rabbit’s foot
- Blowing on a dandelion
- Throwing salt over our shoulder while spinning around on one leg doing a rain dance
Although noble, these things historically have not worked.
SOT: A New Weapon Against a Formidable Enemy
Fast-forward to today, Lyme disease is no longer just a mysterious illness shrouded in conspiracy theories; it’s a target in the crosshairs of cutting-edge science. One of the most promising new treatments is something called Supportive Oligonucleotide Therapy (SOT)—a precision tool designed to silence Borrelia at its core.
Here’s how it works: SOT involves synthesizing a custom strand of nucleic acid that pairs with the pathogen’s mRNA, effectively disabling its ability to reproduce. It’s like a molecular sniper, locking onto its target and shutting it down before it can wreak more havoc. Unlike antibiotics, which can cause collateral damage to your microbiome, cause our bug to go into hiding, and sometimes fail entirely, SOT is pathogen-specific, attacking Borrelia without disturbing the rest of the body’s ecosystem.
SOTs for chronic infections, like Lyme, were developed by Research Genetic Cancer Center or RGCC’s lab about 20 years ago now. They are made 100% specifically tailored to your unique strain of Lyme or Bartonella, or Epstein Barr, or whatever. They don’t make them for everything, but they do make quite a few…:
- 19 strains of Borrelia
- 6 strains of Bartonella
- 6 strains of Babesia
- Anaplasma
- Rickesttia
- Ehrlichiosis
- HHV1/HSV1 – (Human Simplex Virus – Oral-Facial)
- HHV2/HSV2 – Herpes Simplex Virus – Genital)
- HHV6 (A & B) – Human Herpes Virus – 6
- CMV – (Cytomegalovirus)
- Coxsackie Virus (Type A & B)
- VZV – Varicella Zoster (shingles)
- EBV – Epstein-Barr Virus
- HPV- (16/18) – Human Papilloma Virus
- HPV- (6/11) – Human Papilloma Virus
- HBV – Hepatitis B Virus
- HCV – Hepatitis C Virus
- HIV – Human Immunodeficiency Virus
- HTLV1 – Human T-Cell Lymphotropic Virus
The SOTs work like Velcro. They bind to the replication section of the virus, making it unable to replicate or divide. No replication equals cell death. Period. This strategy works amazingly well for cancer, too – which is what it was initially developed for. BUT it works even better for these chronic infections. For most people, it’s one SOT infusion per infection and game over.
These little Velcro strips are so tiny and so stealthy that they can find their target even hiding in a biofilm state. It’s like shining sunlight through a window. And they are SAFE. They can only bind to their target. If you make an SOT for Sally and give it to Jake, well, it won’t work.
The word ‘mRNA’ has justifiably gotten a bad rap over the past few years. But SOTs aren’t gene therapy. They can’t touch your genome at all. They can only velcro strip the pathogen (or cancer) that shows up on your individual blood sample.
SOT therapy isn’t new. It’s been around since the 1990s actually. (I was in my 20s in the 1990s – why isn’t that considered new?) Supportive oligonucleotide therapy is also referred to as ‘antisense’ therapy. This is a therapy used for amyotrophic lateral sclerosis (ALS) and spinal muscular atrophy (SMA) and is being studied for use in treating hepatitis C. Not that we necessarily care about what the FDA thinks, recent FDA Approvals in Antisense Therapies include:
Antisense Therapy for ALS (Tofersen)
- Tofersen (brand name Qalsody) is approved for amyotrophic lateral sclerosis (ALS) associated with mutations in the SOD1 gene. Mutations in this gene lead to the production of a misfolded and toxic SOD1 protein, which contributes to motor neuron degeneration.
- Tofersen is an antisense oligonucleotide (ASO) that binds to SOD1 messenger RNA (mRNA).
- By binding to the SOD1 mRNA, it prevents the translation of the toxic SOD1 protein.
- This reduces the accumulation of harmful protein levels and slows the progression of ALS in patients with this mutation.
- Tofersen is one of the first disease-modifying treatments for this specific genetic form of ALS, targeting the root cause rather than just managing symptoms.
Antisense Therapy for SMA (Spinraza)
- Spinraza (generic name Nusinersen) is approved for spinal muscular atrophy (SMA), a genetic disorder caused by a deficiency in the SMN protein (survival motor neuron protein), critical for motor neuron function. This deficiency is due to mutations in the SMN1 gene.
- Humans have a backup gene, SMN2, but it primarily produces a truncated, or broken, nonfunctional version of the SMN protein.
- Nusinersen targets the SMN2 mRNA to enhance the production of the full-length, functional SMN protein.
- This increases SMN protein levels in motor neurons, improving their survival and function.
- Spinraza was the first FDA-approved treatment for SMA and has significantly improved outcomes in infants and children, including motor function and survival.
Why Antisense Therapy Works for These Conditions
Antisense oligonucleotides are highly targeted, allowing them to increase or decrease the production of specific proteins. For genetic diseases, they target the faulty mRNA directly, offering a more precise intervention than conventional drugs.
There are no FDA approved SOTs or antisense therapies for Lyme. Yet. Your genetic Lyme profile is unique to you. The antisense therapies for hepatitis C, ALS, and SMA are one size fits everyone who has that disease type situation. The latter are convenient as pharmaceuticals. The former fix an underlying illness – not the model Pharma is after.
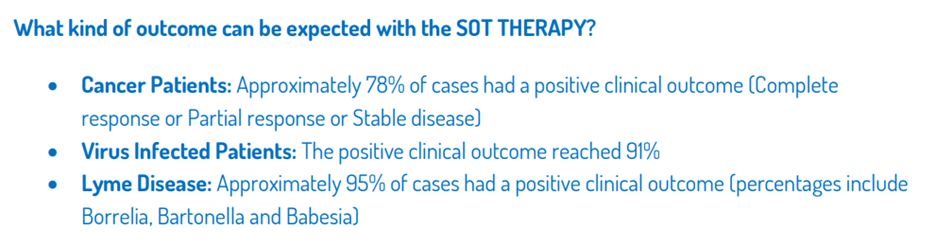
So, of course, SOTs for Lyme are not approved by the FDA, nor are they covered by your insurance. However, they have a 20+ year track record and a success rate greater than 95%. It’s your money.
Risks of SOT Therapy
I don’t want to totally sugarcoat this. I do, actually, because the reported benefits tsunami style dwarf this section. As Borrelia dies off (or cancer cells – we use it for both), it can release toxins that can stress the body’s detoxification pathways, leading to what’s known as a Herxheimer reaction. When Lyme dies off, other co-infections can potentially kick up. This isn’t bad or scary, but it can feel like the flu —worsening symptoms like fatigue, brain fog, and joint pain. Yes, sometimes symptoms can temporarily get worse before they get better. It’s an uncomfortable but necessary step on the path to recovery. Not everyone gets this. Most people don’t, but I’m including it here in the spirit of full disclosure.
Detox support is important to include with SOT therapy. This means bolstering the liver with glutathione, supporting the immune system with vitamin D and vitamin C, and managing inflammation with tools like low-dose naltrexone (LDN), antihistamines, and co-treatment of candida or mold. Optimizing the gut microbiome is also key—because, as we know, 70% of your immune system resides there. Think of it as building an army to help you win the battle. Folks don’t need this full court press situation forever – just on the front end of therapy.
How Many Treatments Will I Need
SOTs are given as a brief intravenous infusion in the doctor’s office. How many SOTs a person needs depends on how many strains of Lyme or other co-infections they have. There are many non-SOT approaches to treating chronic infections that have demonstrated efficacy, but I have never seen significant efficacy with anything other than SOT for Borrelia Burgdorferi. Unfortunately, there are many strains of Borrelia, but only one of them is named after the bioweapons specialist. Just saying.
Not unlike Covid, Lyme variants often need a beat down, just like the original variant. So, to answer the question, typically, just one SOT is needed for Borrelia Burgdorferi, but most patients elect to treat all notable strains. Sometimes that’s one, sometimes it’s seven. But once previous infections are gone, >95% of the time, they’re gone.
For decades, Lyme disease has been the El Chupacabra of infections. Evasive, shape-shifting, antibiotic defying, crippling. Conventional and functional medicine interventions aimed at eradicating Lyme disease have largely failed. Until now. For the first time ever, we have something that works. SOT therapy brings hope to countless numbers of men, women, and children whose lives have been devastated by this catastrophic tick-borne illness.
Conclusion: The Lyme Conspiracy Lives On
The story of Lyme disease is as bizarre as Borrelia itself—an insidious bacterium that behaves like a bacteria, a virus – let me check the wind direction. Emerging near a secretive Cold War bioweapons facility and causing decades of suffering for untold numbers of people. Whether you believe in the conspiracies or not, the facts remain: Lyme disease is real, it’s devastating, and for many, the conventional system has failed to offer a cure.
But for the first time, I finally feel there’s hope. With innovative therapies like SOT, we’re seeing breakthroughs that would’ve been unimaginable just a decade ago. We’re not just managing symptoms anymore; we’re targeting the root cause. And for those who’ve spent years battling chronic Lyme, that’s nothing short of revolutionary.
So, was Lyme disease the original lab leak? Or is Covid the better story? The answer may forever remain a mystery. But as we unravel the science, the medicine, and the history, one thing is clear: the truth—like Borrelia—may be buried deep, but it’s worth digging for.
And for you folks on the east coast, you don’t need to worry about the animal research facility on Plum Island. It was officially closed down in December 2024. That biosafety level 4 facility studying animal and plant diseases that could be dangerous to humans has been relocated – to Kansas:)
That’s going to do it for me. If you found this video informational or entertaining, please like the channel, subscribe and share it with a friend. Those things really help get the channel out. Until next time, stay hopeful, keep learning, because in the end, it is you who are in charge of your own health care. We’ll see you for the next one. Bye for now.
https://www.cdc.gov/lyme/treatment/index.html
Case Report: PANDAS and Persistent Lyme Disease With Neuropsychiatric Symptoms: Treatment, Resolution, and Recovery
https://pmc.ncbi.nlm.nih.gov/articles/PMC7884317/
Bitten: The Secret History of Lyme Disease and Biological Weapons, Kris Newby
Lab 257: The Disturbing Story of the Government’s Secret Germ Laboratory, Michael C Carroll