
Nothing like starting things off with a bang, right? This isn’t a clickbait post aimed at drawing a strike for the channel or spreading misinformation. It’s about shedding light on an important medical and scientific topic that affects tens of millions of women in this country. A topic that should be extremely nuanced but instead has become something… different. Something that looks and sounds a lot like dogma. I’ve talked about this before. Remember, dogma isn’t science. It isn’t discourse or debate. Dogma is religion. When something is believed so strongly, so absolutely, it is no longer argued by dissenting viewpoints or new data, we call it dogma.
The need for and benefit of annual screening mammography has become medical dogma. It’s been wrapped up by industry, stamped with the approval of ‘insert three letter agency here’, and put into medical textbooks never to be discussed ever again.
Shut up science deniers. This conversation is over.
“Mammograms save lives.”
“Mammography is the most accurate method of breast cancer detection.”
“Mammograms use a very small amount of radiation, which is considered safe and outweighed by the benefits of early detection.”
How many times have you heard these statements? I’ve been hearing them since medical school – fast becoming a distant memory. And I believed them. I know we’re well past October, but the incidence of breast cancers could care less. Women are being diagnosed with more aggressive breast cancers at younger ages than ever before in recorded history. A trend that has taken a dramatic turn upward in recent years.
My patients with breast cancer used to be older than 60. Postmenopausal at least. Then they were younger. Women in their 50s. Then women in their 40s. Those women were almost universally recipients of a genetic variant unknown by their mothers or sisters. The infamous BRCA gene. But occasionally they weren’t. Then the women were even younger. In their 30s, their 20s. Ever hear of a 20 something year old woman presenting with stage 4 breast cancer? I have. Now…
The debate about why these cancers are happening is taking place quietly in the shadows of platforms where you can safely ask such questions. Certainly not FB and YT so, sorry, we won’t be hashing that out here. Well, maybe a little bit. Later.
Whatever the cause, the panic is real. And if the horrifying kinds of breast cancers are truly on the rise, the question being shouted from the rooftops is an obvious and sensical one:
Women, have you had your screening mammogram?
Like most things in conventional medicine, breast cancer treatment is a one-size-fits-all type situation. Regardless of almost every factor and demographic, we treat women diagnosed with breast cancer the same way we did in the 1950s. We cut it out, radiate the area, and then potentially treat it with chemotherapy. Surgery is scary, painful, and disfiguring. Radiation causes cancer. It can kill cancer but causes it too. Chemotherapy is poison. Period.
If we treated breast cancer with chicken soup and herbal tea, overdiagnosis wouldn’t be an issue because chicken soup and herbal tea are benign interventions. They don’t hurt anyone. Unless you’re allergic to herbs. Or chicken. But that’s not what we do. We cut, we radiate, and we poison cancer. If a person has a life-threatening malignancy, the risk incurred by that strategy may very well be worth it. But what about breast lesions detected on mammograms that never would have become clinically relevant disease? Is it worth it for those women?
Conventional breast cancer treatment leaves women with hair loss, bone loss, brain loss, vaginal dryness, no libido, no energy, higher rates of cardiovascular disease and dementia. Higher risk for other types of cancer. If treatment doesn’t buy you at least an extension of life expectancy, is it worth enduring all of this? Can that even happen? Can the diagnosis of breast cancer be….wrong? Sure it can.
Let’s get into it.
The Mammogram Debate
I know I’m going to get hate from this post. I can hear it already.
“If I skipped my mammogram last year, I never would have known I had breast cancer.”
“If my sister hadn’t done her yearly mammograms, she would have died from breast cancer.”
“My mother had a normal breast exam with her doctor, so without the mammogram, they would have missed her breast cancer.”
OK, I heard you. I totally hear you. The argument I am going to make isn’t whether or not mammograms can detect breast cancers, in some cases before they would be detected on clinical exam. Although I will argue they miss as many if not more than they catch. My argument is whether or not these mammogram detected cancers would ever have needed treatment to begin with – and whether the risk of the radiation exposure from the annual boob squeeze is outweighed by this benefit.
In any other situation, people fairly uniformly agree that radiation is a bad thing. There’s a hole in the ozone layer. The dentist puts a 50-pound lead blanket on your chest before taking an x-ray of your molars. You’re limited as to how many CT scans you can have done in a calendar year. All of this because we agree that radiation carries risk. Slap a pretty name on it, color it with pink ribbons, and suddenly ‘mammograms’ are considered something different. What?
The Canadian National Breast Cancer Screening Study
I want to first call attention to the data here. One of the largest studies published to date on the efficacy of screening mammography was the Canadian National Breast Screening Trial published all the way back in the early 1990s. Before ‘science’ was officially and unequivocally co-opted by special interest. This randomized control trial followed close to 90,000 women aged 40 to 59 for almost 25 years.
The authors randomly selected 45,000 women to receive annual breast cancer screening with mammography. The other 45,000 women did not receive mammograms. Some of these women did self-breast exams, some had clinical exams done by their doctors, and some of them did nothing. In comparing women who did to those who did not have annual mammograms, they found absolutely no difference in breast cancer mortality.
To restate: mammogram or not, the exact same number of women in both groups died from breast cancer.
They did, however, find a difference between the two groups of women. There was a 20-30% higher rate of breast cancer diagnosed in the women ‘screened with mammograms’ group compared to the control.
- More cancer diagnosed in the mammogram group.
- Same number of women died from breast cancer – mammogram or not.

Canadian National Breast Screening Study: 1. Breast cancer detection and death rates among women aged 40 to 49 years
A B Miller, C J Baines, T To, C Wall
https://pubmed.ncbi.nlm.nih.gov/1423087/
The Nordic Trials Cochrane Report
The Nordic Trials show these same findings but on an even larger scale. The “Nordic trials” in the context of mammogram breast cancer screening refer to a series of large, randomized controlled trials conducted in several Nordic countries, most notably Sweden, which studied the effectiveness of routine mammogram screening in reducing breast cancer mortality among women.
The review published in 2013 includes seven trials that involved 600,000 women aged 39 to 74. 300,000 women were randomized to receive annual screening mammograms, the other 300,000 were not. Here again, there was absolutely no mortality benefit in the mammogram group. The same number of women died from breast cancer whether they had annual screening or not.
Like the Candian study, these trials also showed a 30% higher incidence of breast cancers diagnosed in the mammography group compared to the controls. So, it’s difficult to ever say with certainty that a mammogram saved someone’s life. We can say that screening will result in some women getting a cancer diagnosis even though their cancer would not have led to death or sickness. But would they ever became ill from that diagnosis? Would it have simply gone unknown and been quiet until they left this dimension for some completely unrelated reason?
When we look at the actual statistics, they go like this:
- For every 2000 women we screen annually with mammograms, we may potentially save one life.
- However, in so doing, we will cause 10-20 women to be victims of the diagnosis of breast cancer and treat them unnecessarily.
- Additionally, more than 200 women will experience significant psychological distress, anxiety, and uncertainty for years because of false positive findings.
These are numbers worth seriously considering.

Screening for breast cancer with mammography
Peter C Gøtzsche, Karsten Juhl Jørgensen
https://pubmed.ncbi.nlm.nih.gov/23737396/
I used to be of the mindset that breast cancers behaved predictably. Catch it early, treat it aggressively, and we’ll have the best in terms of outcomes. I don’t believe this any longer. It’s an overly simplistic view of an incredibly complicated disease state. Cancer is a metabolic disease that causes extremely variable gene expression when, if measured, tells us how that cancer is going to behave and how best to treat it. extremely variable gene expression when, if measured, tells us how that cancer is going to behave and how best to treat it. More on that in a bit.
Why Is There So Much More Breast Cancer?
Crappy Living
One could argue that for decades, we’ve been living with an unacceptable incidence of breast cancer. All cancer, really. We eat toxic food, use toxic products, and generally live toxic lives. OK sure – all of those things matter, and we can collectively do a better job of mitigating those risks.
- Clean up diet – eat real food
- Avoid xenoestrogens like those in plastics, pesticides, and unfiltered water
- Use safe personal and household products
- Minimize exposure to fake hormones like those in birth control pills and conventional HRT
Unfortunate Genetics
There is the risk associated with certain genetic factors, like BRCA gene mutations that run in families. But although the overall incidence of breast cancer is increasing, the incidence of specifically BRCA-associated breast cancer is not. We have better detection capabilities now than we did in the past, but the actual occurrence of these cancers is not increasing in the population at large. And cancers associated with specific gene mutations still represent a relatively small percentage of the overall breast cancer population.
These factors all play a role in risk. But do they explain this? Data from the UK showed a relatively predictable rate of breast cancer until just recently. Newly published disability data demonstrates a 48% and 40% increase in new excess clearances for breast cancer claims in 2022 and 2023.
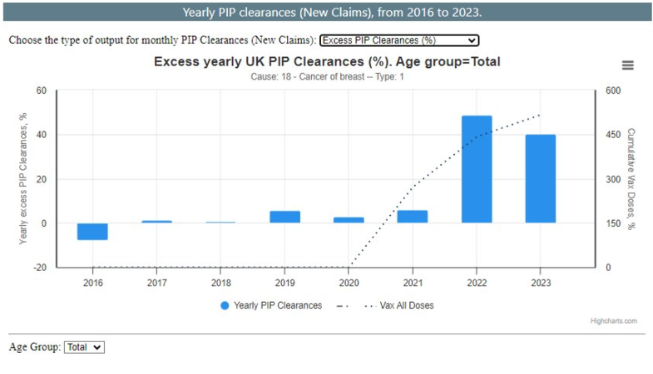
And what about this? Excess death rates from breast cancer in the UK were 5% in 2020, then rose to 12% in 2021, and 28% in 2022.

Humanity Projects
https://phinancetechnologies.com/HumanityProjects
You could argue that we all have cancer cells floating around in our bodies all the time. It’s our immune system’s job to police that situation and keep it in check. ‘Hey wait a minute – who’s that bad guy over there? Take that dude out.’ Dendritic cells, T lymphocytes, natural killer cells all come together to keep cancer cells from taking hold.
There are lots of things that can contribute to an excess burden on our immune system, our police force, per se, that can negatively impact its ability to maintain peace and order. I’m going to call out the two biggest offenders: chronic infections and that other thing which shall not be named.
Immune System Dysfunction
During a relatively recent pandemic, there was a relatively new therapeutic that was injected into a relatively large percentage of the global population that may or may not have been studied long enough to know whether it would or would not have had detrimental effects on our immune system function. Or any other function for that matter. Three years into this global experiment, we now know it most certainly does. We know the mechanisms, we know the pathways, we know the predisposing factors. And immune system dysregulation all the way from autoimmune disease to cancer is at an all-time high.
Chronic infections also heavily tax our immune system function – and there’s a whole bunch of these. Parasitic infections, Candida, Lyme, and other tick-borne infections are bogging down our police force allowing cancer cells to sneak in the back door. We see evidence of this from regular blood testing. Check out your last CBC or complete blood count. Is your overall WBC or white blood cell count low? Has it always been and your doctor tells you, there’s nothing to worry about? That’s just your normal?
Are your monocytes, eosinophils, or basophils high? I bet any money you’re dealing with some sort of chronic infection. Those subtle changes don’t necessarily tell us which infection it is, but it means we’d better look now, or we’ll be finding something even worse later on.
Breast Cancer Screening Alternatives to Mammography
Thermography
Thermography is a non-invasive technique that uses infrared imaging to detect changes in temperature and patterns of blood flow seen in the very early stages of cancer development. Infrared imaging is an FDA-approved adjunct to mammography that can detect thermal abnormalities associated with breast cancer. One of the primary benefits of thermography is its lack of radiation exposure to the patient. This makes it similar to ultrasound and contrary to conventional mammography. Additionally, it is non-invasive, meaning there is no contact with the breast during imaging.
Ultrasound
Ultrasound is another non-invasive technique for cancer screening which doesn’t utilize ionizing radiation or compression. Typically used as adjuvant to other screening modalities, studies suggest that ultrasound has greater sensitivity and accuracy for detecting breast cancer than mammography in certain populations of women. Shaped by tissue density, the transmitted sound waves create the images seen by ultrasound which can guide further diagnostics or biopsy. Unfortunately, most hospitals and clinics will not perform breast ultrasound in the absence of a concurrent mammogram, regardless of a woman’s choice to omit the radiation.
Magnetic Resonance Imaging (MRI)
MRI uses powerful magnets, radio waves, and a fancy computer to produce extremely high-resolution images of soft tissues in the body, without any radiation. Despite their obvious advantages, breast MRIs unfortunately have some concerning risks of their own – specifically their requirement for contrast dye.
In order to capitalize on the full advantages MRI has to offer, gadolinium containing ‘contrast’ is routinely administered prior to the procedure. Gadolinium is a heavy metal which has well documented ties to severe kidney damage in certain patient populations and long-term tissue deposition in the brain and other soft tissues. In 2007, the FDA issued its infamous Black Box Warning on the use of gadolinium. A Black Box Warning is the most serious type of warning issued by the FDA alerting users to be extremely cautious in weighing the potential risks versus benefits before use.
Additionally, breast MRI is also exponentially more expensive than traditional mammography – on average 10x more – and typically not covered by insurance companies.
Self-Breast Exams (SBEs)
Women aren’t typically fans of examining their own breasts, but they should be! 60% of breast cancers are found by the women who own them. Those of us who have them, should really get to know them. You can set a reminder on your calendar or phone and check in with your breasts on a monthly basis – preferably the week after your period, if you’re still having those. If you’re not, ‘feel them on the first’ of each month.
RGCC Next Generation Liquid Biopsy
I’ve written recently on this, so I’ll include a link to the different tests offered by Research Genetic Cancer Center or RGCC’s blood testing for cancer below. RGCC, located in Florina, Greece, offers cutting edge therapeutics and test options for cancer. This is blood testing, ladies. So, no boob smashing. This is the cat’s ass of cancer screening as far as I’m concerned. A yearly blood test to evaluate for the presence of basically any type of cancer? No radiation, no colon prepping, no invasive exam? I’m in.
RGCC testing doesn’t just tell us whether a woman has breast cancer or not. It profiles the cancer, telling us all its little secrets about how it behaves metabolically and genetically as well. This allows us not only the benefit of supremely early detection, but the ability to individually tailor cancer intervention based on the unique profile of a person’s cancer.

RGCC’s Next Generation Cancer Testing Elevating the Cancer Paradigm To a Superior Standard
Quantitative Transmission (QT) Imaging
So, this is new and fun. My nurse refers to this type of breast imaging as ‘boob in a bowl’. It really is. You lay on your stomach on a fancy table and your boob goes in a bowl of nice warm water and it just sits there. QT imaging is a type of ultrasound imaging, specifically utilizing “quantitative transmission ultrasound” technology to create true 3D images of the breast. It’s safe. It’s fast. It’s painless.
Because QT imaging uses ultrasound, it does not involve ionizing radiation. The high image resolution allows for visualization of even significantly dense breast tissue. These images have incredibly high resolution and can be repeated in close sequence to follow suspicious lesions over time, potentially reducing the need for additional imaging or biopsy in some patients. By providing detailed tissue information, QT imaging may enable earlier detection of suspicious lesions, potentially leading to earlier diagnosis and treatment of breast cancer.
However, however, however, like conventional ultrasound, QT imaging is not recognized as a standalone screening tool for breast cancer. There are no scanners nearby if you happen to be in my neck of the woods. And the equipment is on the spendy side – trust me I’ve looked into it. If anyone wants to crowd fund this, please hit me up in the comments. We’ll name the breast cancer center after you:)


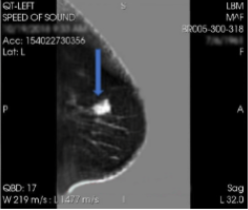

QT uses sound waves transmitted through a water bath which provides a true 3D image of the breast. It’s safe. It’s fast.

Conclusion
Mammography has long been the mainstay for breast cancer screening. Since its introduction in the late 1970s, mammography has been strongly recommended by physicians, cancer organizations, and our public health officials. Once reserved for women with significant risk factors, today mammography is recommended annually or biennially for most women aged 40-75.
Despite the extensive use of routine mammograms, deaths from breast cancer continue to rise and many studies demonstrate there is no mortality benefit from mammography whether you have them routinely or never at all. The sensitivity of this screening modality is dramatically diminished in women with dense or fibrocystic breasts. Mammography involves compressing the breast with 42 pounds of pressure between two plates. It only takes 22 pounds of pressure to rupture the encapsulation of a cancerous tumor. Not a fan of those numbers either.
Today we went over many of the arguments against universal screening with mammography due to false positives, false negatives, and psychological stress, but my biggest criticism outside of lack of mortality benefit is that mammograms are x-rays of the breasts. X-rays are radiation. Radiation causes cancer. I know you all know this, but in plain English, this test uses something that causes cancer to find cancer. I have had mammograms in the past, but I don’t plan to have another because I believe there are better options available.
Thermography, ultrasound, liquid biopsy with RGCC’s next generation cancer sequencing are all superior screening tools in my opinion. When we get the ‘boob in a bowl’ I’ll add it to the list😊
I don’t necessarily believe that mammograms are a scam or that the system was designed to purposefully put women in harm’s way by recommending this type of screening. The doctors recommending mammograms and the techs performing them are largely good people who believe they are doing a good thing. But sometimes in science we need to pause and re-evaluate our processes and protocols. Sometimes findings tell us a different story, or a different technology proves to be better.
It would be in everyone’s best interest to take that pause now – because I think we’re all due for some major changes.